As a veteran neonatal nurse and lactation consultant, I am often asked by parents to explain how the antibodies found in breastmilk work to protect their babies. Published research on immunology is extremely technical and difficult to understand, and unfortunately, the information that is readily available (especially on social media) contains a lot of false and conflicting information. So I’m here to share evidence-based information about this very important topic in a way that is easier for most parents to understand.
Our immune system is very complex, but generally speaking, it is responsible for fighting off both germs that enter our bodies from our environment, and also for protecting us from diseases like cancer that occur within our bodies. I will be focusing on how the immune system fights off germs, which it does by producing antibodies.
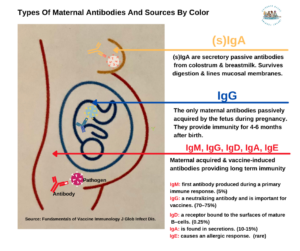
An antibody is a protein that is produced by the body’s immune system when it detects the surfaces of foreign and potentially harmful substances, also known as pathogens. Examples of pathogens are bacteria, fungi, and viruses, which are all microorganisms. The antibody response is specific; it will seek out and neutralize the microorganism and stop the invasion. There are five classes of antibodies: IgM, IgG, IgA, IgD, and IgE.
Thank you for your Twitter post raising the very important topic of stress, guilt, and sadness when a breastfeeding mother experiences low milk production.
I could feel the deep despair you expressed through your words because I have supported thousands of mothers, just like you, who felt tremendous guilt and stress when they tried their best to make enough milk.
Can I emphatically tell you something? You and your body did not “fail” with making enough milk. You were failed by the current breastfeeding education and guidelines, which don’t fully inform mothers about their biological and psychosocial risk factors for low milk supply. Instead, parents are taught that every mother can make enough breast milk if she has the right support; but the research tells us that low milk supply is far more common than people realize. All of the support in the world cannot increase breastmilk supply if your body cannot biologically produce it!
Unfortunately, breastfeeding promotion and education has placed an ominous label on formula milk in hopes of increasing breastfeeding rates as part of the public health campaign of “Breast is Best.” Countless mothers have told me they were terrified to even use formula, even when they knew their baby was hungry and they didn’t have enough breast milk. Mothers are repeatedly told that “being fed formula is the bare minimum,” or formula is depicted as junk food, sometimes even by lactation consultants. I have blogged about these mothers’ horrific stories countless times to bring attention to this critically important matter. This mother took a letter from her psychiatrist to take to the hospital to protect her from being shamed for formula feeding her newborn. This mother had a suicide plan, and this mother attempted suicide from the relentless pressure to exclusively breastfeed. This mother took her life. According to her grieving husband, the relentless pressure to exclusively breastfeed played a key part in her tragic decision.
Formula milk is being depicted as ‘junk food’ by a lactation consultant.
Mammary physiology is not exempt from dysfunction, just like all other organ functions in our bodies. The largest study ever done to measure actual breast milk production was done by Kent et al. in 2016 following 116 breastfeeding mothers with and without breastfeeding problems. The mothers measured all the breast milk they fed their infants over the first month of life through direct feeding (using weighted feeds) and expressed breast milk feeding. This study found that between days 11 and 13, 2/3rd of the mothers could not produce more than the minimum 440 mL required to feed their infant exclusively and between 14 and 28 days, nearly 1/3rd could not produce that minimum.
This means that some mothers will not make enough breast milk and will need to use formula milk to nourish their babies so they thrive! Formula milk is based on the components of breastmilk and is nutritionally balanced to meet a baby’s dietary requirements.
No mother should be ashamed for using it because low milk supply is—and always has been—a struggle that some mothers face, through no fault of their own.
Breastfeeding has been strangely transformed to represent an idealized image of the most perfect, loving and best mother possible on social media by aggressive breastfeeding zealots. But a baby doesn’t bond with breastfeeding or formula feeding—a baby bonds and thrives on being fed with love by present loving parents.
Research has confirmed that a baby doesn’t bond with breastfeeding or formula feeding—a baby bonds and thrives on being fed with love by present loving parents.
Formula feeding stigma may have negative effects on maternal and infant well-being. Results provided the first experimental evidence of formula feeding stigma; the formula feeding mother was viewed less positively than the identical breastfeeding and control mothers, who were typically not perceived differently than one another.
These results imply that caregivers, health care providers, and policy makers should be mindful of the potential for pro-breastfeeding rhetoric to be associated with formula feeding stigma (with potential consequences for the health of women and infants) and consider implementing interventions designed to reduce stigma and promote awareness of the safety and utility of proper formula use.
This study below suggested that negative public responses cause a mother to feel guilty for using infant formula and result in negative feelings of self-worth and dysfunctional maternal behaviors.
This mom could not biologically produce enough breastmilk to meet the exclusivity standards and felt like she was failing her baby. We supported her with our team of clinical experts and she went on to mix feed her baby knowing she was not a failure and her baby was not being fed substandard nutrition.
Ms. Teigen, your breastfeeding and formula feeding experience didn’t have to turn out like this, and I am so sorry you experienced sadness, stress, and guilt. Because of moms like you, who couldn’t find real support for shame and judgment-free infant feeding, I co-founded The Fed Is Best Foundation almost five years ago with my partner, Dr. Christie del Castillo-Hegyi. Dr. Christie launched our foundation by sharing her story about her delayed onset of breastmilk which hospitalized her son for life-threatening complications of unintended starvation while trying to exclusively breastfeed. You may have heard about the story of Jillian Johnson, whose baby boy Landon died from insufficient breastmilk intake–all to avoid ONE drop of formula milk.
We desperately need your help to destigmatize the shame and guilt related to formula feeding.
We would be honored if you would consider joining our #fedisbest advocacy team so that together we can bring awareness to the public to support all safe infant feeding with breast milk, formula, or a combination of both, eliminate infant feeding shaming while prioritizing perinatal mental health. Thank you for considering!
With warm regards,
Jody Segrave-Daly, MS, RN, IBCLC
Christie del Castillo-Hegyi, M.D.
Our mission statement: The Fed is Best Foundation works to identify critical gaps in current breastfeeding protocols, guidelines, and education programs. We provide families and health professionals with the most up-to-date scientific research, education, and resources to practice safe infant feeding with breast milk, formula, or a combination of both. To be fully informed, parents must be taught the risks of insufficient breast milk intake when supporting exclusive breastfeeding in order to prevent hospitalizations for insufficient feeding complications. Finally, we strive to eliminate infant feeding shaming while prioritizing perinatal mental health.
Contact Us
Fundraising Group. Please send an email to Jody@fedisbest.org if you are interested in joining any of our volunteer groups.
If you need infant feeding support, we have a private support group– Join us here.
If you or your baby were harmed from complications of insufficient breastfeeding please send a message to contact@fedisbest.org
Make a donationto the Fed is Best Foundation. We are using funds from donations to cover the cost of our website, our social media ads, our printing, and mailing costs to reach health providers and hospitals. We do not accept donations from breast- or formula-feeding companies and 100% of your donations go toward these operational costs. All the work of the Foundation is achieved via the pro bono and volunteer work of its supporters.
Sign our petition! Help us reach our policymakers, and drive change at a global level. Help us stand up for the lives of millions of infants who deserve a fighting chance. Sign theFed is Best Petition at Change.org today, and share it with others.
Share the stories and the message of theFed is Best Foundation through word-of-mouth, by posting on your social media page, and by sending our FREE infant feeding educational resources to expectant moms that you know. Share theFed is Best campaign letter with everyone you know.
Print out our letter to obstetric providers and mail it to your local obstetricians, midwives, family practitioners who provide obstetric care and hospitals.
Write to your local elected officialsabout what is happening to newborn babies in hospitals and ask for the legal protection of newborn babies from underfeeding and of mother’s rights to honest informed consent on the risks of insufficient feeding of breastfed babies.
Send us your stories. Share with us your successes, your struggles, and everything in between. Every story saves another child from experiencing the same and teaches another mom how to safely feed her baby. Every voice contributes to change.
Send us messages of support.We work every single day to make infant feeding safe and supportive of every mother and child. Your messages of support keep us all going.
Shop atAmazon Smile and Amazon donates to Fed Is Best Foundation.
Or simply send us a message to find out how you can help make a difference with new ideas!
For any urgent messages or questions about infant feeding, please do not leave a message on this page as it will not get to us immediately. Instead, please email christie@fedisbest.org.
Thank you and we look forward to hearing from you!
Parents are taught that it’s normal for babies to lose 7–10% of their body weight in the first few days after birth, but is this true? Well, that depends. According to the AAP, a baby who loses more than 7% of his body weight may be losing excessive weight and requires a comprehensive lactation evaluation to rule out delayed onset of copious milk production, primary lactation failure, and/or infant oral anomalies that prevent adequate colostrum/milk transfer.
Weight loss has typically been assessed using simple percentages, but now there is a much more precise and accurate way to track excessive weight loss in newborns and many hospitals, pediatricians, and lactation consultants are adopting this method for greater accuracy in making clinical recommendations.
The Newborn Weight Tool, or NEWT, is an online tool, the first of its kind, to help pediatricians determine whether exclusively breastfed newborns have lost too much weight in the first days of life. The tool was developed at Penn State College of Medicine through research conducted jointly with University of California, San Francisco. It was developed using a research sample of hourly birth weights from more than 100,000 breastfed newborns. For a quick synopsis of this tool from the lead investigator and one of developers of the tool, Dr. Ian Paul, watch the video below.
In this video, Dr. Ian Paul, professor of pediatrics and public health sciences at Penn State College of Medicine and pediatrician at Penn State Hershey Children’s Hospital, talks about how NEWT fills an important void. Determining whether an exclusively breastfed newborn is losing excessive weight is important because higher weight loss almost always reflects suboptimal milk intake. It is also associated with increased risk of medical complications such as low blood sugar, jaundice, and dehydration, which can result in the need for medical interventions and future health and developmental problems. This weight-loss tool shows that how quickly babies lose weight is just as important as how much they lose.
HOW TO USE THE NEWBORN WEIGHT LOSS TOOL
We recommend practicing using the Newborn Weight Loss Tool before delivery to become familiar with how it works. We have provided a few examples here to help you practice using the tool. We encourage all parents to ask their health care providers for the numbers they need (birth weight and follow-up weights in grams and time of weighing) to use this tool. Along with the Fed is Best Infant Feeding Plan, the NEWT provides parents with the confidence they need to meet their breastfeeding goals while meeting their infant’s nutritional needs safely. If you are having trouble using the NEWT resource, you may reach us at contact@fedisbest.org for assistance. For urgent medical concerns regarding your infant, please contact your pediatrician’s office.
The first step is to record the weight in grams and time of the weighing each time it is done at your health facility, starting with the birth weight. The Fed is Best Feeding Plan has a helpful chart to help you record all weights and other clinical data.
Please note the weight time entered is in military time. Click here to convert the time to military time.
Please click here to convert pounds/ounces to grams which are used in the hospital.
Mode of feeding: either exclusive breastfeeding or exclusively formula-feeding.
If you are giving formula exclusively or supplementing breastfeeding with formula from the first feeding, choose exclusive formula-feeding
Vaginal or Cesarean Delivery
Then the next weighing after the birth weighing
When you submit the data, the tool will plot the weight loss data on a graph. Weight loss greater than the 75th percentile (or below the yellow line on the graph) is considered to be excessive weight loss and requires an urgent assessment of the breastfeeding technique and of the newborn for signs of jaundice, dehydration, and other conditions to determine the need for supplementation.
With this tool, excessive weight loss can be detected earlier. Previously 7% weight loss was believed to be normal and safe for all newborns but if they lose this amount in the first 24 hours, this would be considered excessive weight loss that is greater than what is lost by 95% of all exclusively breastfed newborns. This may be a sign of insufficient breast milk supply and/or poor transfer of milk. Supplementation with milk bank donor milk or formula would be strongly recommended at this time if the correction of the latch is unable to stabilize the weight loss. Earlier detection and supplementation can prevent complications that could require hospital interventions and longer hospital stays. Alternatively, the tool may provide mothers reassurance that their infant is getting sufficient breast milk and that supplementation may not be needed at this time.
Keep in mind that the choice to supplement is a decision that is ultimately up to the mother, regardless of the findings of this weight loss tool. Choosing to supplement just to relieve the hunger of a persistently hungry newborn or to prevent maternal exhaustion are all valid reasons to supplement a baby. Furthermore, the best evidence available has shown that judicious supplementation after nursing sessions will not harm a mother’s chances of going on to exclusively breastfeeding thereafter may even prevent need for repeat hospitalization. Furthermore, contrary to prior claims, early supplementation in this study found no effect on the gut microbiome as previously claimed.
This weight loss example is well within normal limits, confirming that breastfeeding is going well.
NOW LET’S LOOK AT AN EXAMPLE OF HOW THE NEWT TOOL SUPPORTS SUCCESSFUL BREASTFEEDING WHILE PROTECTING THE BABY FROM EXCESSIVE WEIGHT LOSS AND THE HUNGER AND THIRST THAT ACCOMPANY IT.
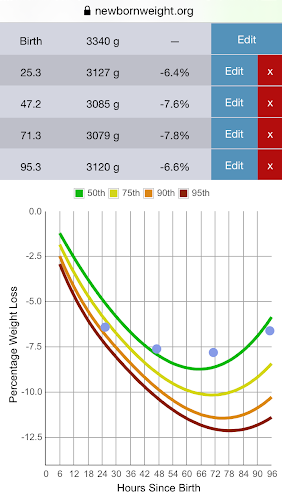
This baby, born by c-section at 37+4 weeks, weighed 3340 g (7 lb 6 oz) at birth. His mother was exclusively breastfeeding and was concerned that he was not getting enough milk. She reported that he would fall asleep at the breast after a few sucks, and would cry and show hunger cues when put down. The pediatrician was concerned because of the baby’s high 24-hr weight loss (>75th %ile) and the fact that his nursing sessions were so short and infrequent due to sleepiness. She recommended that the mother supplement with formula and ordered a lactation consult.
The lactation consultant helped this mother hand express and pump several milliliters of colostrum. She then worked with the mother and baby to breastfeed with a syringe of colostrum and banked donor milk slipped into the corner of his mouth. With the presence of a faster flow, the baby stayed awake for the whole feeding and then appeared satisfied after taking about 18 ml. The mother was given a milk expression plan to ensure adequate stimulation of her breasts while waiting for the arrival of her milk. When her milk came in on Day 4, the baby’s weight loss was still in the normal range (6.6%, around the 50th %ile), and she worked with an outpatient lactation consultant to return to exclusive breastfeeding.
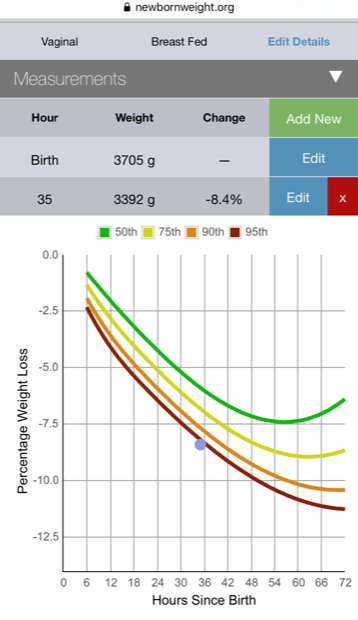
NOW LET’S LOOK AT AN EXAMPLE OF HOW THE NEWT CAN DETECT EXCESSIVE WEIGHT LOSS.
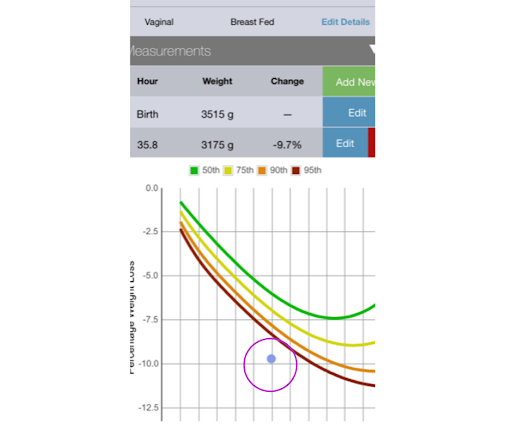
This baby lost 8.4% of his birth weight at 36 hours. No supplementation was offered. Thirty-six hours later the family found out at his follow-up appointment that his weight loss was down to 9.7% and his transcutaneous bilirubin was very high, and they had to send a blood test. The mother of the child, a physician at the hospital where she delivered stated, “The crazy thing about all of this though, was that since he had not lost over 10% of his birth weight, they did not insist on supplementation. But the lab test resulted in immediate readmission for bili lights. His total bilirubin was 21.” From the blog: Hospital Drops Baby-Friendly Program After Doctor’s Baby Was Harmed
THIS IS ANOTHER EXAMPLE OF HOW NEWT CAN DETECT EXCESSIVE WEIGHT LOSS.
This baby had a 9.7% weight loss at 36 hours of age. Using the NEWT tracking tool, this baby had excessive weight loss at discharge—he had lost much more weight than 95% of vaginally born babies—but no interventions were suggested.
This baby was not scheduled for a follow-up pediatrician appointment until 36 hours later. Unfortunately, by the time this baby was seen in the ER, the weight loss was greater than 22%. He did not survive.
This baby was failed by the arbitrary guideline that 10% weight loss is acceptable for all babies. In addition, this baby should have been seen by the pediatrician the very next morning, which is another systemic failure. We believe if all parents use the NEWT resource, they will have immediate access to determine if their baby needs supplementation and if the mother needs lactation management. The truth is that very often babies are sent home hovering at 7–10% weight loss, putting them at risk before the onset of copious milk production. Because of this, we advocate for all discharged exclusively breastfed babies to have a next day exam and weight check by their pediatrician.
Although the Newborn Weight Loss Tool is far superior to the previous arbitrary standard of 10% weight loss as being normal, there are some limitations. The tool is the summary of average newborn weight loss in exclusively breastfed babies across a population and therefore cannot fully capture what is going on with an individual infant. As we know, statistical data on a population cannot replace the judgment of the mother and health professionals seeing an individual newborn who may be communicating that despite what appears to be a normal weight loss, they are persistently hungry and that supplementation may still be needed to prevent feeding complications. Weight loss percent is not sufficient to rule out all feeding complications. This may require further clinical evaluation like a blood glucose, bilirubin or metabolic panel, which may cause transient discomfort to your baby but may be important to ensure safe and adequate feeding.
Unfortunately, some feeding complications can occur before 7% weight loss is reached, including hypoglycemia and hypernatremia, a form of severe dehydration that can cause brain injury and increased risk of death. Studies shows that hypernatremia can occur by 5% weight loss, more typically at weight loss greater than 7% of birth weight. The data also shows that among healthy exclusively breastfed newborns, hypoglycemia and the complications it causes to the brain can occur at any weight loss percentage, because some infants are born with low caloric stores. That is why it is important to listen to the baby, first and foremost, and secondly; to all the health professionals reading this, listen to the mother when they are concerned that their newborn is not getting enough milk.
Any newborn with signs of persistent HUNGER (which we have summarized in this article) deserves a full assessment of these hunger cues, clinical signs of dehydration, jaundice, and hypoglycemia which may require blood work, particularly when the weight is above 5–7%. We encourage all mothers to listen to their instincts and raise concerns about their infants when they exhibit persistent signs of hunger despite frequent breastfeeding. In many cases, supplementation can help your infant become more alert and effective at breastfeeding, which may encourage breast milk to come in more robustly and reduce the need for further supplementation.
Jody Segrave-Daly is champion for debunking pseudo-science in the infant-feeding community and a staunch advocate for educating mothers about safe breastfeeding in the first days of life, because of the significant number of babies with excessive weight loss and failure to thrive she manages in her private practice. Jody is a 30 year career NICU nurse, Infant Feeding Specialist, and IBCLC. She is a feeding advocate for breastfeeding, bottle feeding, combo-feeding, formula feeding, pumping and tube feeding because she believes supporting mothers individual feeding needs, is much more important than advocating a single feeding method. She is known for her shame and judgment free infant feeding consultations, while prioritizing perinatal mental health across the globe. She provides mothers with current evidence base recommendations while tapping into her extensive neonatal nursing and feeding experience, to help parent’s make the best infant feeding decision that works for them.
When I was pregnant, I was determined to breastfeed. It was going to be easy, it was going to be natural. Formula was for lazy people, formula was for selfish women. Formula was poison for my baby. The breastfeeding groups I joined on Facebook only reinforced these mantras even further. Whenever people asked if I was going to breast or bottle feed my baby, I proudly told them that I was going to breastfeed. Nothing was going to stop me. I had no idea how ignorant I truly was.
All the odds were stacked against us from the get-go. The day after my baby was born, the pediatrician assessed her in the hospital and brought it to our attention that she had a severe tongue-tie and that it would need to be revised if I didn’t want to have any pain while breastfeeding. There was an Ear, Nose & Throat specialist on call that was able to do the procedure that afternoon, so we agreed to go through with it. Before her tongue was revised she had a good, strong latch- painful for me, but strong. When they brought her back after the procedure, everything was off; her suck was weak and disorganized and she no longer knew how to use her tongue to suck correctly. Being a first time mother, I had no idea how breastfeeding worked and I had no idea it could possibly take days for your milk to come in.I had my baby over the weekend and since there was no lactation consultant available until Monday I pleaded with the nurses to help me. I kept telling them that something was wrong and that she wasn’t latching on like she was before. They assured me that everything would be okay and that my milk would come in soon.Upon discharge, the nurse handed me the standard goody bag and put a case of formula in there ‘just in case’ breastfeeding didn’t work out. I cringed at the thought of having to use it.
Once we were home, I did nothing but try and establish a successful breastfeeding relationship. It’s all we did. Even though we nursed around the clock, she was hungry, screaming, and frustrated. I decided to cave and put some formula in a syringe to drop while breastfeeding in the hopes of enticing her to latch on better. It seemed to satisfy her a little bit but she still wasn’t latching on. On her first checkup with the pediatrician, we learned that she had lost 1lb 1oz. I expressed my concerns about my milk not feeling like it had come in. He was concerned about the weight loss but never once mentioned the option to stop exclusive breastfeeding, he just told me to keep trying and that my milk would come in. He gave me the number of a lactation consultant and told me to come back for a weight check in a few days.
I live in small town and this lactation consultant was the only one in the area. For whatever reason (to this day I will never know) she refused to meet with me. I begged and pleaded for a home or office visit; she would only text me and suggest things like a nipple shield or trying different nursing positions. I was stubborn, and figured if she wouldn’t meet with me it must mean our issues were not that big of a deal and that me and my baby could figure it out on our own. Weight check after weight check, my baby teetered back and forth at the same weight. On top of her feeding issues, my baby also had acid reflux. I tried to express to the doctor that all we were doing was nursing around the clock and all she
was doing was spitting it back up; the doctor just told me to keep putting her at the breast and that I was overreacting about her amount of spit up.
It wasn’t until she was four weeks old and was screaming a piercing, pterodactyl-like scream that I got scared and knew something needed to be done. I met with a different pediatricianwho took one look at her and told me I needed to take her straight to Children’s Hospital for evaluation. She was diagnosed with the dreaded ‘Failure to Thrive’.
We were in the hospital for four days. I was instructed to breastfeed for thirty minutes, followed by two ounces of formula, followed by me pumping for fifteen minutes. I was to do that every three hours. I was exhausted. I was the kind of exhausted where I was talking to doctors and having no memory of the conversation immediately after it happened, and they expected me to go home and follow this same routine every three hours if I wanted this breastfeeding relationship to work.
So, that’s what I did for the next two weeks, and I went insane. Literally insane. My husband was afraid to go to work and leave me home with the baby, but I continued on because that’s what I thought was best for the baby. I finally found a highly recommended IBCLC an hour and a half away in Lexington, KY and scheduled a consult with her. We did a weigh-feed-weigh and found I was only giving about 20 ml of milk in a thirty minute feeding. She also brought to my attention that my daughter’s tongue-tie that was revised the day after she was born was done incorrectly and that she also had a lip tie which was never mentioned before. My baby had a bite-bite-bite-swallow pattern of eating instead of a suck-swallow-suck-swallow because she didn’t know how to suck properly. She was burning more calories trying to eat than she was actually taking in, and, because she was biting more than sucking, my milk supply had been close to nothing this whole time.
I was referred to a specialist in Louisville, KY to get the tongue and lip revised properly as well as a speech therapist to work on her suck. It took my baby six weeks to get back up to her birth weight. For the next month I put myself through torture trying to nurse, bottle feed, and pump – because that’s what I thought was best for my baby. Eventually I decided I couldn’t do it anymore, but I wasn’t quite ready to give up on breastfeeding, so I decided to supplement. Except this time I was going to formula feed first and supplement with breast milk, instead of the other way around. We continued this relationship for about two months, gradually decreasing our breastfeeding sessions and increasing formula intake until it just hit me one day… that I wasn’t doing this for her – I was doing this for me, and at her expense. We were no longer breastfeeding because it was what was best for her, we were breastfeeding because I was trying to prove that I still could. I wasn’t enjoying my baby. All this time, I hadn’t been bonding with my baby.
I needed to throw in the towel, because that truly, was what was best for her. Since we’ve ended our breastfeeding journey, we’ve both never been happier. I am enjoying her and bonding with her like I never did before. You don’t need to breastfeed to bond with your baby, you need a happy healthy mother and a happy, healthy baby. That’s it. That is a mistake that I will NEVER make again.
Kathleen, a #FedIsBest advocate. #SafeBreastfeeding
Sarah is one of our supporters at The Fed is Best Foundation and she sent us her infant feeding story. Did you know that 17 percent of working women are exclusive pumpers?
Sarah writes:
Long before I was even pregnant with my first, I knew I wanted to breastfeed. Little did I know that that would mean exclusively pumping. When my daughter was born I literally tried everything to nurse her but she would not latch. We struggled (and I cried) for weeks before I finally accepted pumping as my only means of breastfeeding. It worked for us and we went with it. 10 months later I have reached my goal of providing enough milk for her entire 1st year! Exclusive pumping wasn’t easy, but it was worth every minute and every single ounce to me. I’m so thankful I could do this for her, and I’ve never been more proud of anything in my life.
The most important thing I’ve learned is whether you nurse, pump, formula feed (or a combination of the 3), we’re all doing our best to feed our babies, and they love us either way! #FedisBest Sarah~
Please consider supporting our Fed is Best Foundation( Fed Is Best)so that we can continue supporting all familiesin the way they feed their babies while providing the best, evidence -based infant feeding resources in the world!
Donate now and you will receive our #FedIsBest charm to wear in honor of the way your baby was fed. Thank you! Co-founder, Christie & Jody






















You must be logged in to post a comment.